
Access to quality healthcare plays an important role in maintaining overall wellbeing and managing health concerns early. Trusted Doctors in Bundoor...
When it comes to car maintenance, one of the most important things every vehicle owner should understand is the difference between a minor and a maj...

Superannuation is an essential part of financial planning in Australia. It is designed to provide individuals with income during retirement, helping...

Alpine Resorts Victoria (ARV) has welcomed funding support from the Victorian Government’s Tiny Towns Fund, with both Mt Hotham and Mt Buller se...

Security is a critical concern for homeowners, businesses, and vehicle owners alike. Whether it involves protecting a property, replacing damaged lo...

Cavities and minor tooth damage are common dental problems that can worsen if left untreated. Professional tooth fillings help restore damaged teeth, ...

Operating a vehicle safely requires an immediate, uncompromised stream of visual information from the surrounding road environment. A driver's decis...

Planning for retirement requires careful financial decisions, and many Australians are now looking for more direct control over how their superannua...

Professional retail cleaning services are an essential part of maintaining a welcoming, safe, and professional environment for customers and staff...

Selling or leasing a commercial property isn’t just about listing the square metres, taking a few photos and waiting for the right person to appea...

A café display fridge does a lot more than keep cakes cold and sandwiches fresh. It quietly shapes the way customers browse, the way staff move beh...

A great backyard doesn’t need to be huge, expensive or perfectly styled. Most of the time, the spaces people actually use are the ones that feel e...
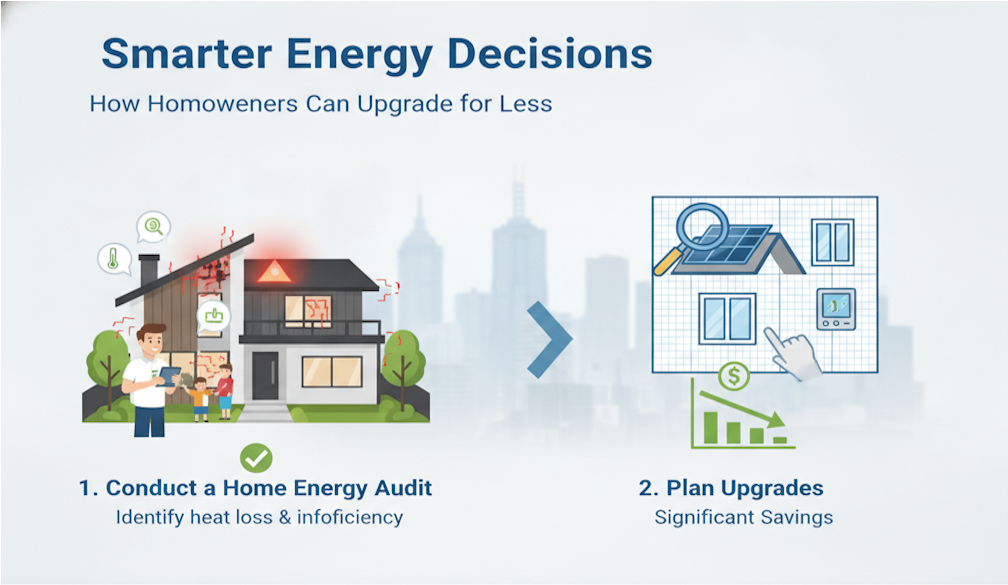
Energy upgrades used to feel like something you only looked into after a power bill gave you a nasty surprise. These days, though, more homeowners a...

Retail customer experience has become one of the most important drivers of revenue growth, especially during high-intensity sales periods. However, ev...

If your only experience of "Indian food" is butter chicken and garlic naan, South Indian cuisine is going to feel like discovering an entirely new c...

A home's roof and drainage system work together every day to protect the property from water damage. While many homeowners focus on visible areas such...

For a small one-off job, an experienced builder can size up the materials in their head. The problem is that most jobs are not small one-off jobs, and...

They say the kitchen is the heart of a house which means a clutter-free kitchen not only makes your home in general look nicer, it also makes cookin...


 Shutterstock
Shutterstock